0 42 Sounds a Bit Rushed Feel Like U Can Continue the Flow With Something Shortened
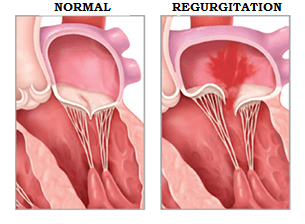 Mitral Regurgitation is basically a leaky mitral valve. It's also known as mitral valve regurgitation, mitral insufficiency or just MR for short. Look at the image of the mitral valve below. The mitral valve separates the top and bottom of the left side of the heart (the main pumping chamber). Usually, the mitral valve stops blood from going backwards and keeps blood going forwards to the body where it is needed. In mitral regurgitation, blood is allowed to leak backwards into the upper chamber of the heart.
Mitral Regurgitation is basically a leaky mitral valve. It's also known as mitral valve regurgitation, mitral insufficiency or just MR for short. Look at the image of the mitral valve below. The mitral valve separates the top and bottom of the left side of the heart (the main pumping chamber). Usually, the mitral valve stops blood from going backwards and keeps blood going forwards to the body where it is needed. In mitral regurgitation, blood is allowed to leak backwards into the upper chamber of the heart.
At myheart.net we've helped millions of people through our articles and answers. Now our authors are keeping readers up to date with cutting edge heart disease information through twitter. Follow Dr Ahmed on Twitter @MustafaAhmedMD
Follow @MustafaAhmedMD
How common is Mitral Regurgitation?
Mitral regurgitation becomes more common with age. This is because of age-related wear and tear of the valve. In the population as a whole around 2% of people have at least moderate mitral regurgitation. In those younger than 40 years of age, it is likely only around 0.5% and in those over 75 years of age it likely approaches 10%. Of course, these estimates are only for moderate or more mitral regurgitation and based on the US population. If we include mild mitral regurgitation this number would be much greater.
Different Types of Mitral Regurgitation
Imagine the valve to be like a double door of a closet, where both doors meet in the middle. If it closes properly blood won't go backwards, if it doesn't close properly then blood will leak backwards. Mitral regurgitation can be classed as primary or secondary. In primary mitral regurgitation, there is a problem with the valve itself (like one of the closet doors being defective). In secondary mitral regurgitation, there is a problem with the structures that surround the valve (like the door frame being too big so the doors don't meet in the middle leaving a gap). In secondary MR often an enlarged heart leads to the valve not being able to meet in the middle.
Trivial, Mild, Moderate, Severe and Torrential Mitral Regurgitation
Based on information from the ultrasound scan of the heart (echocardiogram) the mitral regurgitation can be classified according to its severity.
- Trivial mitral regurgitation is an essentially normal finding and of no concern.
- For moderate and greater mitral regurgitation, there are several features of the heart scan that are taken together to determine the severity.
- In moderate mitral regurgitation around 30% of the blood in the heart is leaking backwards.
- In severe mitral regurgitation about 50% of blood in the heart is leaking backward.
- In torrential mitral regurgitation the majority of the blood is going backwards, this happens in conditions such as flail leaflet.
Causes of Mitral Regurgitation
As explained above, there is primary mitral regurgitation where the valve leaflets are affected and there is secondary mitral regurgitation where the structures holding the valve in place are affected.
Primary mitral regurgitation where the valve leaflets are affected.
- Mitral Valve Prolapse. The most common cause in the US is mitral valve prolapse. In mitral valve prolapse, the leaflets become thickened and spongy and if severe can lead to leakiness through the valve. Click here for a detailed article regarding mitral valve prolapse and regurgitation.
- Chord Rupture. Sometimes the chords, which are the strings holding the valve in place, can snap rendering that part of the valve ineffective. A rupture of a large chord can lead to a condition known as flail leaflet, leading to torrential mitral regurgitation, described here in detail.
- Mitral Valve Endocarditis. Endocarditis is an infection within the valve that directly destroys the valve tissue. This basically leads to a hole being eaten out of the valve and the leak occurs through the hole.
- Rheumatic Fever. This starts with a strep throat infection and years later can lead to damaging the valve due to a reaction in the body that causes it to attack its own valve. This used to be the most common cause in the US although it has now significantly declined due to early treatment of strep infections. Rheumatic heart disease still remains one of the most common causes of mitral valve disease in developing countries. Rheumatic heart disease leads to hardening and limited function of the mitral valve and can cause both narrowing and regurgitation so the valve is too tight and also too leaky!
- Valve Calcification. As we age there can be degeneration of the heart valves, similar to the way in which joints degenerate. In some cases, this degeneration can deform valve leaflets and interfere with valve function leading to regurgitation.
- Drugs. Although much less common now, there have been drugs used in the past, such as weight loss, or migraine headache medications that were found to cause damage to the valve leaflets. These drugs are ergot alkaloids (methysergide and ergotamine), ergot-derived dopaminergic agonists (such as pergolide and cabergoline) and drugs metabolized into norfenfluramine (such as fenfluramine, dexfenfluramine and benfluorex).
Secondary Mitral Regurgitation, also known as Functional Mitral Regurgitation where the structures holding the valve in place are affected.
- Heart failure / Cardiomyopathy. In some conditions that lead to heart failure the heart enlarges and the heart function decreases. The heart can sometimes enlarge so much that the mitral valve leaflets cannot meet in the middle and allow blood to leak backwards.
- Coronary Artery Disease. The coronary arteries supply blood to the heart muscle, including the muscles that control the function of the mitral valve. If the blockages are severe then the heart muscle can fail and lead to a process called remodeling. This remodeling of the heart can distort the mitral valve and lead to malfunction and regurgitation.
- Heart Attack Complication – There are two large muscles in the heart known as papillary muscles that are each associated with one of the mitral valve leaflets. In a heart attack, the blood supply to these muscles can be compromised causing dysfunction and valve regurgitation. Rarely the heart attack can lead to rupture of one of these papillary muscles and basically leave one of the mitral valve leaflets free hanging leading to torrential mitral regurgitation.
- Hypertrophic Cardiomyopathy – In this condition there is a severe thickening of the heart muscle. This can often lead to very turbulent flow in the heart that actually leads to distortion of the mitral valve with every beat and can be associated with significant mitral regurgitation.
Risk Factors for Mitral Regurgitation
A lot of the risk factors for mitral regurgitation are related to the causes above.
- Age is the most obvious risk factor; the elderly are at highest risk.
- Those with a history of mitral valve prolapse and regurgitation are at risk of their disease progressing, The higher the degree of mitral regurgitation the more likely it is to progress.
- Normal cardiovascular risk factors such as blood pressure and cholesterol may be important as they can lead to coronary artery disease and heart failure which in turn is associated with heart enlargement which can lead to mitral regurgitation.
- Intravenous drug use increases the risk of endocarditis, an infection in the heart that can damage the valve and lead to regurgitation.
- Certain genetic diseases such as congenital heart disease in which people can be born with defective mitral valves or hypertrophic cardiomyopathy can lead to an increased chance of significant mitral regurgitation.
How Does the Heart Handle Mitral Regurgitation
In mitral regurgitation, blood is leaking from the bottom chamber of the heart back to the top chamber of the heart. It's important to realize that all this blood still has to go forward into the bottom heart with the next beat. So basically in mitral regurgitation the heart has to handle more blood. We call this volume overload. They way the heart handles this extra blood is to grow larger to be able to handle the increased volume of blood. The process of enlargement is known as adaptive remodeling. This is both good and bad. It's good because it allows the heart to handle the extra blood so despite the leakiness, enough blood still goes forward to the body where it is needed. Unfortunately in the process of enlargement the heart muscle becomes weaker over time and eventually fails if not treated in time. That becomes all the more important in the treatment of severe mitral regurgitation. To complicate matters even further, the leakiness allows the pumping function of the heart to appear higher than it actually is. For this reason, it's important to keep a very close eye on how the heart is pumping when there are moderate or greater amounts of mitral regurgitation.
Symptoms of Mitral Regurgitation
Acute Mitral Regurgitation. Rarely, people present with severe mitral regurgitation that happens all of a sudden. Such as in chordal rupture or papillary muscle rupture. This is known as acute severe mitral regurgitation and is a medical emergency. Patients with acute severe mitral regurgitation will present with:
- Low blood pressure
- Shortness of breath
- Dizziness
- Passing out
- Acute severe mitral regurgitation is life threatening and needs to be treated almost immediately.
Chronic Severe Mitral Regurgitation. This is much more common and basically means the disease is present for years and typically progresses slowly. Valve disease is usually clinically silent for many years and may only be picked up by the presence of a murmur. This is because as described above the heart adapts to mitral regurgitation by growing larger. Ultimately, however, in severe disease, the heart fails and the following symptoms may be present.
- Fatigue
- Shortness of breath
- Decreased exercise tolerance
- Leg swelling
- Irregular heart beat
Tests and Diagnosis of Mitral Regurgitation
Auscultation
This is listening with a stethoscope. In mitral regurgitation, there will be a murmur that lasts throughout the whole of the pumping phase. This is the noise made by the blood leaking backward. It is known as a pan-systolic murmur, or sometimes a late-systolic murmur.
EKG Heart Tracing
- This is not the best test for diagnosis of mitral regurgitation but may give some clues as to the effect on the heart.
- In severe mitral regurgitation, there may be an irregular heartbeat known as atrial fibrillation; this can be picked up on the EKG.
- Enlargement of the top and bottom chambers of the heart may be seen in chronic severe mitral regurgitation. Up to 50% of patients will have EKG evidence of left ventricular chamber enlargement known as hypertrophy.
Chest X-Ray
This is not particularly useful, however, a chest x-ray may show signs of congestion and signs of heart chamber enlargement.
Echocardiogram
- This is basically the test of choice in diagnosing mitral regurgitation and is indispensible.
- Echocardiography can be used to determine the underlying cause of the mitral regurgitation, and provide important information regarding the heart chamber size and the integrity of the valve leaflets in addition to the structures holding the valve together.
- Echocardiography is generally considered the most accurate way of determining the severity of mitral regurgitation.
Transesophageal Echocardiogram – TEE
- The TEE is the most accurate test in assessing mitral regurgitation.
- This is an ultrasound of the heart that requires a small tube being passed into the food pipe to get closer pictures of the heart. The advantage being that it shows the structures in greater detail.
- A TEE may be performed to assess mitral regurgitation that is questionably severe and can identify the exact cause of the mitral regurgitation.
- Most people would perform TEE prior to consideration of surgery, and a TEE is almost always performed in surgery to ensure the valve is repaired.
Heart Catheterization
- In this procedure small tubes are passed into the heart to get information about pressures in the heart and also to look at the coronary arteries.
- Heart catheterization can be performed to see the effect the mitral regurgitation is having on the heart.
- Heart catheterization is almost always performed prior to surgery for mitral regurgitation to ensure that there are no artery blockages that would need fixing at the same time.
Magnetic Resonance Imaging
- Although not used as mainstream, some expert centers use this to monitor the progression of mitral regurgitation and the effect it has on the heart, as it gives superior information on the structure and function of the heart.
- One of the advantages is that it is highly reproducible and so it may be of use in cases where close monitoring is important.
Complications of Mitral Valve Regurgitation
Heart Failure
As the heart enlarges to cope with the increase volume of blood it eventually fails, this usually only happens in the setting of severe MR. One of the keys of treatment is to fix the valve before heart failure sets in and to prevent irreversible damage.
Atrial Fibrillation
The large volume of blood that leaks back into the top chamber of the heart in mitral regurgitation can lead to an irregular heart rhythm that originates in the top chamber known as atrial fibrillation. If uncontrolled it is known as Afib with RVR.
Pulmonary Hypertension
Pulmonary hypertension is the term for increased pressure in the arteries of the lungs. It can occur in mitral regurgitation from the back transmission of pressure from the left chambers of the heart that are dealing with the increased blood volume.
Medical Treatment of Mitral Regurgitation
For severe mitral regurgitation, especially if primary and symptomatic, then fixing the valve is the only way to alleviate the problem. There is currently no medicine that can fully reverse the condition. Some medical treatment may be beneficial, as discussed below.
Primary Mitral Regurgitation
- In primary mitral regurgitation where there is a problem with the valve itself such as mitral valve prolapse there is no medicine proven to reverse the disease, and no specific medicine recommended by the guidelines.
- There is some evidence that beta-blocker medication such as metoprolol can have a beneficial effect in terms of preserving the heart function, however the evidence for this is not strong enough to be making it a strong recommendation.
- Measures should be taken to ensure adequate control of blood pressure as increased blood pressure may lead to increased severity of mitral regurgitation.
- Basically the mainstay of medical management is surveillance, monitoring for stability of disease with clinical visits, and echocardiography, ensuring the disease doesn't progress too much before considering valve surgery.
Secondary Mitral Regurgitation
- In secondary mitral regurgitation the problem is not with the valve itself, but rather the structures that hold the valve in place and keep it functioning. Unlike primary mitral regurgitation, medicines may have a significant impact on secondary mitral regurgitation.
- Some cases of secondary mitral regurgitation are caused by coronary artery disease that leads to certain areas of the heart not pumping as well, leading to valve dysfunction. In these cases fixing the coronary artery disease, either through medicines, stents, or surgery may be beneficial.
- Secondary mitral regurgitation is often due to heart enlargement, whereby the heart becomes to big for the valve leading to leakiness. In these cases, medicines that can possibly reverse this process in some way, will allow the heart to become smaller and possibly restore valve competency.
- Measures should be taken to ensure adequate control of blood pressure as increased blood pressure may lead to increased severity of mitral regurgitation.
When to have surgery for Mitral Regurgitation?
When to have surgery for primary mitral regurgitation?
Primary mitral regurgitation is when the valve itself is affected such as in mitral valve prolapse. There is no proven medical therapy to make the valve better and the only way to get rid of the mitral regurgitation is by mitral valve surgery. The options are mitral valve repair and mitral valve replacement, which are discussed later in detail. The timing of mitral valve surgery for mitral regurgitation has been the subject of much debate over the years. When deciding to send someone for valve surgery we have to consider the following. We don't want to send someone too early because heart surgery is a big deal, and if they don't need it then it's hard to justify the risk no matter how small. On the other hand, we don't want to send someone too late because there is the chance that any damage done would be irreversible.
Years ago patients with severe mitral regurgitation would be send for surgery only when the heart showed clear evidence of failure. It was then realized, that many patients would never recover their function and remain symptomatic. So the valve was being fixed too late. The problem is that due to the nature of the condition, it is often hard to know when the heart is reaching that point of failure. Unlike other conditions we can't just rely on the pumping function of the heart to tell us what's going on because in mitral regurgitation it initially looks normal and we often only find out its abnormal after the valve is fixed! For this reason, in severe mitral regurgitation, if the pumping function of the heart is at all reduced, even minimally, the valve should be operated on. The same goes for patients who have symptoms such as fatigue and shortness of breath.
Many expert centers are now moving towards mitral valve surgery in patients who have severe mitral regurgitation even if the heart is pumping normally and the patient has no symptoms. The rationale for that is 1) The surgery is performed before heart failure sets in to prevent any irreversible damage 2) The modern day risk of mitral valve surgery in expert hands is minimal and 3) In expert hands it is almost always possible to repair the valve rather than having to replace it. Some centers still prefer what's called a watchful waiting strategy where they watch patients with severe mitral regurgitation closely for development of symptoms or subtle evidence of heart dysfunction.
In addition to development of symptoms of evidence of heart dysfunction, there are a number of other factors associated with worse outcomes in patients with severe MR. Generally if any of these appear then its time to operate. These are an irregular heart rhythm known as atrial fibrillation, and increase pressure in the lung arteries known as pulmonary hypertension.
Surgery in Primary Mitral Regurgitation – Key Points
- Before considering surgery its important to ensure that the mitral regurgitation is indeed severe in nature.
- In expert centers, its reasonable to consider surgery for severe mitral regurgitation even if there are no symptoms and the heart appears to function normally, as long as there is an almost certainty the valve can be repaired rather than replaced.
- In general patients with severe mitral regurgitation should be monitored closely and surgery should certainly be performed if there is development of symptoms or if there is even subtle evidence of heart dysfunction.
- Other indicators which should suggest the need for surgery in severe mitral regurgitation include development of an irregular heart rhythm called atrial fibrillation or the development of high pressures in the lung arteries known as pulmonary hypertension.
When to have surgery for secondary mitral regurgitation?
In secondary mitral regurgitation, the main problem is not the valve itself, but rather structures that hold the valve in place. The main example of this is in people with severely enlarged hearts, where essentially the heart is too big for the valve. Unlike primary mitral regurgitation, medicines may actually be able to help a lot in those with secondary mitral regurgitation. Before considering surgery in secondary mitral regurgitation, there should be effort to maximize medical therapy.
Often those with secondary mitral regurgitation have severely reduced pumping function and so any operation is of course high risk when compared to the generally healthier population with primary mitral regurgitation. It is unclear whether surgery for secondary mitral regurgitation has any effect on long-term prognosis. The goal of surgery for severe secondary mitral regurgitation is to reduce symptoms, so surgery is generally reserved for symptomatic patients.
Surgery in Secondary Mitral Regurgitation – Key Points
- Before considering surgery for secondary mitral regurgitation its important to ensure maximal use of medicines to see if they can improve the mitral regurgitation.
- Surgery for secondary mitral regurgitation is generally reserved for those who remain symptomatic despite medical therapy.
Mitral Valve Repair vs. Mitral Valve Replacement
When undergoing surgery for mitral regurgitation there are 2 main choices, mitral valve repair and mitral valve replacement.
Mitral valve repair involves making modifications to the existing valve that result in elimination of the mitral regurgitation and restore the valve competency. These modifications include addition of artificial chords to stabilize the valve and also addition of a band around the valve to allow it to function normally. In some cases, when the valve is thick and floppy like in mitral valve prolapse, some of the redundant valve tissue may be cut out.
The other option is mitral valve replacement, using either a metal valve or a tissue valve. A metal valve will last generally lifelong although it will require lifelong use of a blood thinning medication such as Coumadin. A tissue valve does not require the use of the blood thinning medication, however will be subject to wear and tear and therefore have a limited life time, maybe up to 10 years after which further procedures may be required.
When possible mitral valve repair is the preferred course of action if it can last in a durable repair. Expert mitral valve surgeons will generally be able to tell if a valve can be repairable based on the echocardiogram done prior to the surgery. Mitral valve repair is considered superior, when possible, because it may result in improved outcomes and greater preservation of heart function. Unfortunately many patients end up with mitral valve replacement, simply because they were referred to surgeons who aren't skilled in repair. This is unacceptable, and is one of the reasons to ensure your mitral valve disease is managed in a truly expert center.
Robotic Vs. Open Surgery for Mitral Regurgitation
The standard way to repair the mitral valve is to do this via a sternotomy, which is the term for sawing the breastbone. Mitral valve repair is complex, and an advantage to an open surgical approach is that the entire valve can be visualized and complex repair performed. Some people would argue that the open approach allows the highest chance of success in a high quality repair. A minimally invasive approach that involves a smaller incision may also be an option.
A handful of specialist centers are offering a robotic approach to mitral valve surgery. Some very skilled and experienced robotic surgeons, of whom there are not too many, are able to perform even complex repairs. The advantage to a robotic approach would be that the incisions are much smaller than that of standard open surgery. If opting for a robotic approach, its important to know the surgeon is highly experienced in this and has a good track record of mitral valve repair.
Keyhole Catheter Based Treatment of Mitral Regurgitation
Incredible advances in technology over recent years has led to the development of a way to fix some mitral valves without having to perform open heart surgery. This is called percutaneous repair of mitral regurgitation and involves the use of small tubes passed up to the heart from the groin. The most widely studied method of percutaneous mitral valve repair is known as the Mitraclip. In the Mitraclip procedure there is a clip applied to the mitral valve leaflets (as can be seen in the video below) that can reduce the amount of mitral regurgitation. The advantages to this procedure include minimal recovery time, and avoidance of surgical risk in those patients that would have been at high risk of surgery. It is felt that although the Mitraclip procedure is effective at reducing mitral regurgitation, it not as effective as standard surgical approaches.
Currently in the US, the Mitraclip is limited to high-risk subsets of mitral regurgitation, basically those patients that are felt to be at prohibitively high risk of surgery. It is also reserved for primary, and not secondary mitral regurgitation for the time being. Trials are ongoing that will establish the role of the clip in wider subsets of mitral regurgitation.
One of the biggest revolutions in cardiology has been the development of a catheter-based treatment of aortic valve disease. This involves implanting a new valve through a small tube and has been wildly successful. Excitingly there is progress being made on catheter-based mitral valve implantation and this is likely to change the field significantly over the next decade.
Can a Pacemaker Help Mitral Regurgitation?
In some cases of secondary mitral regurgitation, different areas of the heart beating out of sync cause the regurgitation. This can be diagnosed using a combination of an EKG heart tracing and an ultrasound of the heart. In these cases, it has been shown that the use of a particular kind of pacemaker known as cardiac resynchronization therapy (CRT) can lead to the improvement of mitral regurgitation both at rest and on exercise. This will not be effective for primary mitral regurgitation.
What Questions to Ask Your Cardiologist If You Have Mitral Regurgitation
- Cause. What is the cause of the mitral regurgitation? Basically is this primary or secondary mitral regurgitation. If so what supports the diagnosis?
- Severity. How severe is the mitral regurgitation? What were the methods used to determine the severity and do the measurements add up? For example if the mitral regurgitation is thought to be severe, is the heart enlarged to reflect this? If not, is it truly severe? On the contrary, if the regurgitation is moderate but the heart is clearly enlarged, is it truly only moderate? Other tests may be required to confirm.
- Stability. In patients being followed up for mitral regurgitation, especially those with moderate or greater disease, has the disease progressed? If so what has been the rate of progression. If there has been rapid progression closer follow-up may be warranted.
- Effects on the Heart. Particularly in those with moderate to severe disease. Is there any evidence of heart muscle dysfunction, even if subtle? Is the upper chamber of the heart, the left atrium enlarged? Is there evidence of increased pressures in the arteries of the lung (pulmonary hypertension)? Is there any sign of heart rhythm disturbance (atrial fibrillation)? In severe disease, these are important as they may indicate the need for mitral valve surgery.
- Strategy. What is the treatment strategy? If being monitored, how often should this be monitored and why? If the disease is severe, then are you going for a watchful waiting strategy or an early surgical strategy?
What Questions to Ask Your Surgeon If Undergoing Mitral Valve Surgery
- Can the valve be repaired rather than replaced? If not why not? In some cases the valve itself isn't amenable to repair, but often people will have mitral valve replacement when they should have had repair instead, simply because the surgeon is not expert in mitral valve repair techniques.
- How experienced is your surgeon in mitral valve surgery? How many do they do per year? What is their success rate for repair? Don't be scared to ask these questions, it's important to have the utmost confidence in your surgeon.
- If the surgeon is taking a robotic approach, what is their experience level? How many cases have they done? How many of their robotic surgeries end up as open operations?
- Ask the surgeon the likely approach to fixing the valve, based upon the information supplied by the echocardiogram.
- Discuss the advantages and disadvantages of a metallic versus a tissue valve in the event that you need a valve replacement procedure.
What Can You Do to Improve Your Chances of a Good Outcome?
- Develop an understanding and take an interest in your condition. Learn as much as you can and take an active role in management.
- For those patients with moderately severe or severe mitral regurgitation keep a track for development of symptoms such as fatigue, shortness of breath, swelling, and an irregular heartbeat. If you develop these discuss this with your doctor when possible.
- Don't get lost to follow up! Ensure you keep a track of your appointment. Make sure you know how often you need to have clinic visits and how often you need echocardiograms.
- See a specialist that is a proven expert in valve disorders and understands the nuances of management of mitral valve disease.
Why it's So Important to see a Dedicated Valve Specialist
I have patients from all over the world come and see me to obtain opinions on their valve disease. Management of valvular heart disease is complex. Expert management relies on knowledge of imaging, structural heart disease, physiology, surgical techniques and newer interventional techniques. As someone who deals with valve disease day in and day out, I find myself using my knowledge of advanced imaging and intervention frequently. These skills are not commonplace in general cardiology and even though guidelines exist to help management of valvular heart disease, very few of these guidelines are based on a high level of evidence and therefore they are far from perfect. Thus in many ways, management of valvular heart disease such as mitral regurgitation is an art form.
For this reason, the current management of valvular heart disease in the US is far from optimal. A good example of this is that a significant proportion of people sent for surgery for mitral valve replacement will get a valve replacement, rather than the preferred valve repair. This is simply because the skill set of the referring physician and the operating surgeon is limited. The development of post-surgical heart failure is also common when, in fact, much of this may have been avoided if patients had been sent for surgery at a more optimal time. Other nuances, such as simply grading the severity of the regurgitation can often be challenging and once again underline the importance of having this managed by experts who are dedicated to valve disease. If this means you have to travel further to see that specialist, then so be it, as in my mind there is no doubt that the benefits of correct management of the disease will be worth it in the long run.
Source: https://myheart.net/articles/mitral-regurgitation/
0 Response to "0 42 Sounds a Bit Rushed Feel Like U Can Continue the Flow With Something Shortened"
Post a Comment